How the right approach ensures safe, enjoyable hot tub use

Hot tubs are unfairly lumped in with pools, as if they are just smaller, warmer cousins—they are not. They are an entirely different species requiring a softer, more patient approach to management. In heavily used hot tubs, the bather load per gallon of water can be up to 100 times greater than in a typical pool. More bathers in less water mean more organic contaminants, driving up chlorine demand, increasing combined chlorine (disinfection byproducts [DBPs]), and leading to odours, complaints, and potential illness. With a bit of time, a heavily used hot tub can quickly become cloudy and develop a foul smell—sometimes bluntly referred to as “people soup.” This is certainly not the kind of impression a facility wants to give.
As with all aquatic venues, sanitization and water balance are separate issues. Sanitization is focused solely on preventing illness. Water balance focuses on preserving equipment’s useful life by preventing scaling and corrosion. The vast majority of aquatic literature focuses on water balance, with little or no mention of preventing illness—this needs to change. A hot tub can look beautiful and still be crawling with Pseudomonas or Legionella if sanitization is not maintained. This is a deep dive into what really keeps people safe.
Recreational water illnesses
The primary focus of every operator and owner must be on safe use. Recreational water illnesses (RWIs) in hot tubs are different from those in pools. There are two primary differences:
1. Users behave differently in pools and hot tubs. In pools, people swim, so their heads are at the waterline, and accidental ingestion is common. However, documented cases show variation in the amount of ingested water by age and between competitive and leisure swimming.1
Gastrointestinal illness in pools is most commonly caused by swallowing water contaminated by fecal matter. In pools with insufficient sanitizer concentration, fecal matter released into the water disperses and is ingested, leading to illness. However, in hot tubs, users are mostly stationary and do not actively move in the water. There is no documented case of gastrointestinal illness associated with hot tubs.
Considering the design of hot tubs, this is an enlightening observation. Hot tub jets produce directional flow rates that can be considered as low-pressure power washers. The concentrated flow can displace fecal residues from bathers, increasing the need for effective water treatment. Since the bather load is higher in hot tubs, the expectation is that the gastrointestinal illness rate should be higher, but it is not; it is zero. The difference lies in user behaviour. Since hot tub users are soaking and not swimming, they are ingesting very little, if any, water. Therefore, they do not become ill from fecal germs.

2. Differences in water temperature and venue design are a key distinction among RWI types. Legionella pneumophila, the bacteria that cause Pontiac fever and the quite serious Legionnaires’ disease, thrives in hot water and is limited by the cooler temperatures of pools. Legionella bacteria cause pneumonia, and these bacteria are inhaled rather than swallowed. The air injection system of hot tubs produces airborne droplets, a few of which are less than 10 microns in diameter and can be carried into the deeper sections of the lungs.
If the sanitizer concentration is insufficient, those droplets become a delivery system for Legionella bacteria. Once in the lung, the bacteria can invade the macrophage white blood cells, leading to Legionnaires’ disease. If not treated appropriately and promptly, the fatality rate can be 40 per cent. The Legionella illness rate in traditional pools is zero. The lack of aerosol-generating water features, coupled with the growth-inhibiting lower water temperatures in pools, is an effective control measure that prevents outbreaks of Legionellosis.
Free chlorine concentration
The absolute minimum free chlorine concentration in hot tubs is 1.0 parts per million (ppm); however, most registered products and public facilities require 2.0 ppm. For pools, a minimum of 1.0 ppm free chlorine is supported by valid field studies.2,3,4 The data on hot tubs is less robust.
One study found high concentrations of Pseudomonas aeruginosa in commercial hot tubs, even at 3.0 ppm free chlorine. Yet, public health officials reported that none of the users experienced any illness. The investigators suggested that concentrations as high as 1,000 Pseudomonas aeruginosa per millilitre of water did not cause human illness.5
A second investigation confirmed that Pseudomonas is considerably less infectious than fecal germs, especially Escherichia coli O157:H7 (E. coli) and Cryptosporidium (Crypto), but did not determine the minimum effective free chlorine concentration.6 Pseudomonas aeruginosa is well known for causing rashes, especially in hot tubs, and has recently been recognized as the leading cause of RWIs.7 Until additional studies are completed, the best practice is to never allow the free chlorine concentration in hot tubs to drop below 2.0 ppm.
Water balance issues
Without automated control, pH levels in hot tubs rise, especially when the jets are running. This is due to alkalinity off-gassing. The air injection system strips all the dissolved gases from the water. Since alkalinity in recreational water is actually dissolved carbon dioxide, the jets rapidly reduce it when those gases are stripped, raising the pH to around 8.3. As pH rises, the sanitizing efficacy of free chlorine decreases due to a shift in equilibrium toward hypochlorite. This is a primary reason why the free chlorine concentration in hot tubs must be higher than in pools.
Proper water balance in hot tubs is slightly different from that in pools. The continuously rising pH in non-automated tubs and the elevated temperature are the two drivers. Calcium ions have reduced solubility at elevated temperatures and pH. Without proper management, it is fairly easy to scale over a hot tub heater, especially if continually shocking with calcium hypochlorite. Overdosing any product in a hot tub will readily impact the overall water balance. Routinely calculating the Langelier Saturation Index (LSI) is more important in hot tubs than in pools. In general, maintaining lower calcium and alkalinity levels helps offset the tendency of elevated temperatures to promote scale formation.
Conflicts in sanitization and water balance
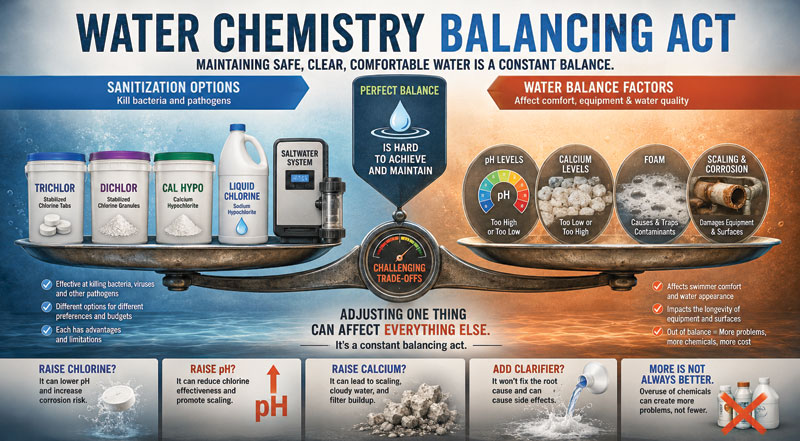
Managing the need for continuous sanitization to control germs while maintaining the correct water balance can lead to conflicting adjustment requirements. Since each type of chlorine has different secondary characteristics, each must be managed differently.
As with pools, the chlorine options include trichloroisocyanuric acid (trichlor), dichloroisocyanuric acid (dichlor), calcium hypochlorinte (cal hypo), sodium hypochlorite (liquid chlorine), and chlorine generated via saltwater systems. No system is perfect, and each of these has advantages and disadvantages. Trichlor is easy to use and provides a consistent feed rate, but it lowers the pH. Dichlor dissolves almost instantly and does not change the pH or increase turbidity. Cal hypo increases calcium concentration and pH and often induces short-term turbidity. Liquid chlorine increases the pH and total dissolved solids (TDS). Salt systems increase the pH. So, which one should be used? Public health authorities generally advise against using trichlor, dichlor, or cyanuric acid in hot tubs.
The chemistry of each product is well-defined and not in dispute. However, the impact of cyanuric acid on sanitization is strongly disputed. The widely cited Centers for Disease Control and Prevention (CDC) recommendation to avoid using any cyanuric acid in hot tubs first appeared as a footnote in the Morbidity and Mortality Weekly Report (MMWR), which described two outbreaks in hot tubs.
Both hot tubs in the report were being operated on cal hypo, but neither was being properly managed. No scientific justification was offered in the footnote.8 There is a theoretical possibility that elevated cyanuric acid reduces the efficacy against Giardia.9 Giardia is a fecal RWI, and fecal pathogens are not an issue in hot tubs.10 Thinking objectively, there is no single best option.
The challenge for the operator is to manage both the advantages and disadvantages of the selected chlorine source and to understand how each chlorine’s secondary properties affect the overall water balance. This can only be accomplished by routinely testing all parameters, not just a quick check of free chlorine and an occasional pH check. Managing hot tubs is not a task for untrained personnel.

Water replacement
Routine water replacement is essential in maintaining a properly sanitized and balanced hot tub. Draining, a quick wipe-down, refilling, balancing, and sanitizing are almost always quicker and less costly than repeated chemical treatments after an extended period of tub use.
The most reliable indicator of usage is the TDS concentration. TDS increase is due to the accumulation of non-volatile ions, such as calcium and sodium, organic compounds, including cyanuric acid, and bather waste, such as perspiration and oils. For service providers, there are easy-to-use handheld meters that read out in a few seconds. Once the TDS concentration exceeds the initial balance concentration by 1,500 ppm, the accumulation is excessive. A more involved method uses the formula: Litres of water in the tub divided by 11.4, divided by the estimated number of bathers per day (Gallons of water in the hot tub divided by three, divided by the estimated number of bathers per day) equals the replacement interval.
The replacement interval is the frequency at which the hot tub should be completely drained and refilled.11 At the very least, residential hot tubs should be drained, cleaned, and refilled every
90 days.

Best practices
Commercial hot tubs (including hotels and health clubs)
- Use an automated chlorine and pH control system managed by a certified operator.
- Manually test the chemistry at least once per day or as required by local regulations.
- Completely drain and replace the water frequently.
- Once the TDS exceeds the initial balanced concentration by 1,500 ppm, it is time for a complete water replacement.
Residential hot tubs
- Check the sanitizer and pH before every use and adjust if necessary.
- Shock the tub after every use.
- If shocking with liquid chlorine or cal hypo, adjust the pH down immediately.
- Drain the tub completely at least every three months and refill it with fresh potable water, then balance it.
All hot tubs
If the tub has not been maintained properly:
- Do not use it and do not turn on jets. There could be Legionella in the water.
- Completely drain the water, flush the systems with a spa purge, refill, rebalance, and add sanitizer before use.
If the foam persists for more than two minutes after the jets are turned off, stop use immediately:
- If the calcium is less than 150 ppm, add calcium and retest.
- If the calcium is more than 150 ppm, the concentration of organic matter is too high. Completely drain the water, flush the systems with a spa purge, refill, rebalance, and add sanitizer before use.
- Persistent foam is from the excess accumulation of organic compounds from bathers. It is concentrated DBPs and germs. Foam is proof that the “people soup” has become quite obnoxious.
- When in doubt for any reason, stop use and check with an expert on the proper treatment. The customer service departments of chlorine and bromine manufacturers are readily available and reliable sources of information.
Notes
1. For more, see Suppes, L.M., Abrell, L., DuFour, A.P., and Reynolds, K.A. 2014. Assessment of swimmer behavior and pool water ingestion. J. Water and Health 12 (2): 269–279.
2. Refer to Esterman, A., Roder, D.M., Cameron, A.S., Robinson, B.S., Walters, R.P., Lake, J.A., and Christy, P.E. (1984). Determinants of the Microbiological Characteristics of South Australian Swimming Pools. AEM 47(2), 325-328.
3. Review Hooker, E.A, Chinn, W.A., Bain, N.C., Busam, G.C., Srirangan, A., & Young, A.R. 2010. Determinants of bacterial contamination in pools, spas, and wading pools: Should chlorine standards be revised? International J of Aquatic Research & Education, 4, 33-38.
4. See also Robinton, E.D., Mood, E.W., & Elliot, L.R. (1957). A study of bacterial flora in swimming pool water treated with high-free residual chlorine. AJPH. 47(9), 1101-1110.
5. Additional insight is provided by Price and Ahearn. 1988. Incidence and Persistence of Pseudomonas aeruginosa in Whirlpools. J Clin Micro. 26(9) 1650-1654.
6. Futher details can be found in Roser, D.J., B. Van Den Akker, S. Boase, C.N. Haas, N. J. Ashbolt, and S. A. Rice. 2015. Dose–response algorithms for water-borne Pseudomonas aeruginosa folliculitis. Epidemiol. Infect. (2015), 143, 1524–1537.
7. For a broader perspective, consult Gerdes et al., 2023. Estimating Waterborne Infectious Disease Burden by Exposure Route, United States, 2014. EID. 29(7) July 2023.
8. For context, see CDC. 2000. Pseudomonas Dermatitis/Folliculitis Associated With Pools and Hot Tubs — Colorado and Maine, 1999—2000. MMWR. 49(48)1087-1091, December 08, 2000.
9. A related study is presented in Falk, R.A., Blatchley, E.R., Kuechler. T.C., Meyer, E.M., Pickens, S.R., Suppes, L.M. 2019. Assessing the Impact of Cyanuric Acid on Bather’s Risk of Gastrointestinal Illness at Swimming Pools. Water, 11, 1314-1337.
10. Industry guidance is outlined in Vore et al. 2018. Recreational Water Illness Handbook. 2018. Pool and Hot Tub Alliance.
11. Operational best practices are detailed in CPO Handbook. 2026. Pool and Hot Tub Alliance.
Author
Dr. Roy Vore is a pool operator, researcher, and instructor specializing in recreational water management, float tanks, and aquatic regulations. He has been a Certified Pool & Spa Operator (CPO) and instructor for more than a decade and has conducted research on microbial control since 1991. Vore has authored more than 100 papers and contributed to industry guidance, including the Model Aquatic Health Code (MAHC) and the Recreational Water Illness Handbook.
Sign up for our newsletter
Get all the latest news and features from Pool & Spa Marketing. Submit your email below to get our twice-monthly newsletter.
Products


Read the Latest Issue